CRESCER CRIANÇA, INFANTIL, JUVENIL: O resultado é uma diferença hereditária na manifestação do gene dependendo se o alelo específico (tem sido conhecido que mutações em regiões não codificantes que afetam a expressão genética possa causar doença genética humana) é herdado da mãe ou do pai. Imprintings (não impressão do código de alelos, a detecção da expressão de genes específica para o alelo em um único indivíduo depende da capacidade para distinguir o produto do gene de um cromossoma parental a partir da outra, e, em seguida, para quantificar as quantidades relativas de cada produto do gene que é produzido. Vários métodos diferentes têm sido descritos e dois desses métodos têm sido utilizados para o levantamento de um número de genes) específicos do alelo são exemplificados por anormalidades do cromossomo 15q11-13, nas quais eliminações dos cromossomos paternos resultam na síndrome de Prader-Willi (SPW) e eliminações do locus materno são associadas à síndrome de Angelman – (esta se caracteriza por atraso no desenvolvimento intelectual, dificuldades na fala, distúrbios no sono, convulsões, movimentos desconexos e sorriso frequente. Além disso, é um exemplo clássico de imprinting genômico causado pela deleção ou inativação de genes críticos do cromossomo 15 herdado da mãe. Sua síndrome irmã é chamada de síndrome de Prader-Willi, sendo causada pela deleção de genes paternos), são duas condições fenotipicamente distintas. Os mecanismos moleculares responsáveis por marca genômica envolvem metilação variável de DNA. A Síndrome de Prader-Willi é uma condição genética complexa que afeta muitas partes do corpo. Na infância, esta condição é caracterizada pela hipotonia muscular, dificuldades de alimentação, crescimento deficiente, e atraso no desenvolvimento. Começando na infância, os indivíduos afetados desenvolvem um apetite insaciável, o que leva a comer em excesso crônico (hiperfagia) e obesidade.
Algumas pessoas com síndrome de Prader-Willi, particularmente aqueles com a obesidade, também desenvolvem diabetes mellitus tipo 2 (a forma mais comum de diabetes). Pessoas com síndrome de Prader-Willi têm tipicamente de leve à moderada deficiência intelectual e dificuldades de aprendizagem. Os problemas de comportamento são comuns, incluindo acessos de raiva, teimosia e comportamento compulsivo, como coçar a pele. Anormalidades do sono também podem ocorrer. Os recursos adicionais desta condição incluem características faciais distintivas, tais como a testa estreita, olhos amendoados e boca triangular, baixa estatura linear, mãos e pés pequenos. Algumas pessoas com síndrome de Prader-Willi têm a pele invulgarmente clara e cabelos de cor clara. Ambos os homens afetados e mulheres afetadas têm órgãos genitais subdesenvolvidos. A puberdade é atrasada ou incompleta, e os indivíduos mais afetados são incapazes de ter filhos (são inférteis). A primeira evidência de imprinting no eixo IGF emerge dos estudos de desregulação do gene alvo IGF-2 em roedores que causou o retardo do crescimento fetal somente quando o alelo desregulado foi herdado do pai (isto é, imprinting materno). O gene IGF-2 fator de crescimento semelhante à insulina-2 é similarmente marcado. Em tecidos onde somente os cromossomos maternos estão presentes, como teratomas de ovário, nenhuma manifestação do IGF-2 fator de crescimento semelhante à insulina-2 é observada, enquanto a manifestação do gene é observada em tecidos onde somente cromossomos paternos estão presentes (mola hidatiforme completa). O gene H19 parece sofrer imprinting de maneira recíproca ao igf2/IGF2, e os dois genes podem ser coordenadamente regulados, de forma que os genes são localizados próximos e no mesmo cromossomo. Os genes para o receptor do tipo II de IGF, que é o mesmo que o gene do receptor cátion-independente de manose-6-fosfato, também apresenta imprinting, mas de maneira diferente.
Assim, o gene do camundongo para o receptor de igf2 e os genes humanos para o receptor de IGF-2 são expressos por alelos maternos (isto é, imprinting paterno). Se o IGF-2 funciona como um fator de crescimento fetal, temos, assim, potencial para a regulação materna e paterna do tamanho fetal. O fator de crescimento semelhante à insulina 2 (IGF-2) é uma proteína de três hormônios que partilham uma semelhança estrutural com a insulina. A definição MeSH lê: "Um peptídeo neutro bem caracterizado supostamente secretado pelo fígado que circula no sangue e tem um regulador de crescimento mitogênico semelhante à insulina e o fator de crescimento tem uma importante, mas não absoluta, dependência de somatotropina (GH-hormônio do crescimento). Acredita-se ser um importante fator de crescimento do feto em contraste com o fator de crescimento semelhante à insulina-1 , que é um importante fator de crescimento em adultos ". Nos seres humanos, o gene IGF-2 está localizado no cromossoma 11p15.5, uma região que contém numerosos genes impressos. O principal papel do IGF-2 é como um promotor de crescimento hormonal durante a gestação. No processo da foliculogênese, o IGF-2, é criado pelas células da teca e atuam de uma forma autócrina sobre as células da teca, e de um modo parácrino em células da granulosa do ovário. O IGF-2 promove a proliferação de células da granulosa durante a fase folicular do ciclo menstrual, atuando ao lado do hormônio folículo-estimulante (FSH). Após a ovulação já ter ocorrido, o IGF-2 promove a secreção da progesterona durante a fase lútea do ciclo menstrual, juntamente com o hormônio luteinizante (LH). Assim, o IGF-2 atua como um co-hormônio, juntamente com o FSH e o LH.

Um estudo realizado no Monte Sinai School of Medicine descobriram que o IGF-2 pode ser ligado à memória e à reprodução. Um estudo da European Neuroscience Institute-Goettingen (Alemanha) descobriu que o medo induzido por extinção a sinalização IGF-2/IGFBP-7 promove a sobrevivência por 17-19 dias de idade, dos neurônios do hipocampo de recém-nascidos. Isto sugere que as estratégias terapêuticas que aumentam a sinalização do IGF-2 e a neurogênese do adulto podem ser adequadas para o tratamento de doenças associadas a um excessivo medo de perda de memória, tais como TEPT (que é o Transtorno de Estresse Pós-traumático (PTSD)). Quando em perigo, é natural sentir medo. Este medo provoca muitas mudanças no corpo em frações de segundo para se preparar para se defender contra o perigo ou para evitá-lo. Esta resposta de "luta ou fuga" é uma reação saudável destinada a proteger uma pessoa do mal. Mas no transtorno de estresse pós-traumático (PTSD), esta reação está alterada ou danificada. As pessoas que têm PTSD podem se sentir estressadas ou com medo, mesmo quando elas não estão mais em perigo. O resumo indica que o comprometimento do IGF-2, na fase de crescimento intrauterino, o IGF-1 na fase pós-natal e a deficiência de GH-hormônio de crescimento, acarretam uma grande disfunção em diversas áreas do metabolismo, não só com deficiência de crescimento em todos os estágios mas também compromete o sistema nervos central, a maturação das fases infantil, juvenil incluindo a fase adulta, e defasagem cognitiva. Por outro lado, o padrão Ouro no desenvolvimento, traduz uma excelente qualidade de vida.
GROWING CHILD-JUVENILE- YOUTH: INHERITANCE POSITIVE AND NEGATIVE FATHERS - IMPRINTING IGF GROWTH FACTOR -LIKE INSULIN.
GROWING CHILD-JUVENILE-YOUTH: THE REGULATION OF GENES FOR IGF GROWTH FACTOR SYSTEM LIKE INSULIN CAN ALSO BE SUBJECT TO GENOMIC IMPRINTING IT IS A PROCESS THAT INFLUENCE A SPECIFIC EXPRESSION OF GENES. CERTAIN GENES ARE ONLY AUTOSSOMAL MANIFESTED FROM A THEORY OF TWO ALLELES AVAILABLE RIGHT OF THIS MODE IS SPECIFIC TO PARENT OF ORIGIN. PHYSIOLOGY-ENDOCRINOLOGY-NEUROENDOCRINOLOGY-GENETICS-ENDOCRINE-PEDIATRICS (SUBDIVISION OF ENDOCRINOLOGY): DR. JOÃO SANTOS CAIO JR. ET DRA. HENRIQUETA VERLANGIERI CAIO.
GROWING CHILD-JUVENILE- YOUTH: the result is an inherited difference in gene expression depending on whether the specific allele (has been known that mutations in non-coding regions that affect gene expression can cause human genetic disease). It is inherited from the mother or father. The imprintings (not printing the code alleles, the detection of the expression of genes specific for the allele in a single individual depends on the ability to distinguish the product of the gene of a parental chromosome from each other, and then, to quantify the amounts for each gene product is produced. Several different methods have been described, and two of these methods have been used for the removal of a number of genes) allele-specific are exemplified by chromosome abnormalities 15q11-13 in which deletions of the paternal chromosomes result in Prader-Willi syndrome (PWS) and deletions of the maternal syndrome locus are associated with Angelman syndrome (it is characterized by delay in mental development, speech difficulties, sleep disturbance, seizures, disjointed movements and frequent smile. Moreover, it is a classic example of genetic imprinting caused by deletion or inactivation of critical genes on chromosome 15 inherited from the mother. Syndrome his sister is called Prader-Willi syndrome, is caused by a deletion of paternal genes), two conditions phenotypically distinct. The molecular mechanisms responsible for genomic variable mark involve DNA methylation.

Prader-Willi syndrome is a complex genetic condition that affects many parts of the body. In childhood, this condition is characterized by weak muscle tone (hypotonia), feeding difficulties, poor growth, and delayed development. Beginning in childhood, affected individuals develop an insatiable appetite, which leads to chronic excess in eating (hyperphagia) and obesity. Some people to Prader-Willi syndrome, particularly those with obesity also develop type 2 diabetes mellitus (the most common form of diabetes). People with Prader-Willi syndrome typically have mild to moderate intellectual disabilities and learning difficulties. Behavior problems are common, including anger, stubbornness and access compulsive behavior, like scratching the skin. Sleep abnormalities may also occur. Additional features of this condition include distinctive facial features, such as narrow forehead, almond shaped eyes and triangular mouth, linear low stature, and small hands and feet. Some people with Prader-Willi syndrome have unusually fair skin and light colored hair. Both affected males and affected women have underdeveloped genitals. Puberty is delayed or incomplete, and most affected individuals are unable to have children (infertile). The first evidence of imprinting the IGF axis emerging from studies of gene targeted disruption of IGF-2 in rodents causing fetal growth dysregulated only when the allele inherited from the father was delayed (e.g., maternal imprinting). The IGF-2 gene insulin-like growth factor-2 is similarly marked. In tissues where only the maternal chromosomes are present as ovarian teratomas, no expression of IGF-2, insulin-like growth factor-2 is observed, whereas the expression of the gene is observed only in tissues where paternal chromosomes are present (spring complete hydatidiform). The H19 gene appears to undergo reciprocal of the IGF-2 imprinting/IGF-2 manner, and the two genes can be coordinately regulated, so that the genes are located close together and on the same chromosome.
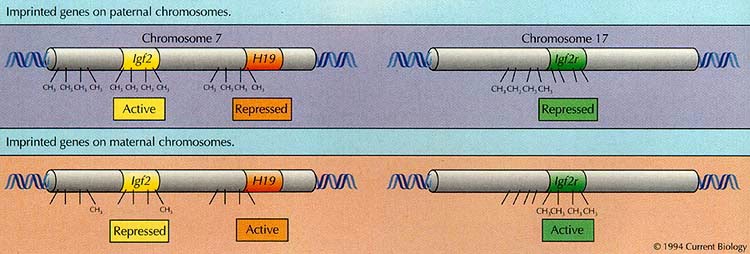
The genes for the receptor type 2 IGF, which is the same as the receptor gene cation-independent mannose-6-phosphate; have also imprinting, but differently. Thus, the gene for the receptor of mouse and human IGF-2 genes for IGF-2 receptor is expressed by maternal alleles (e.g., paternal imprinting). If the IGF-2 functions as a factor in fetal growth and thus have potential for regulation of maternal and paternal fetal size. The Insulin-like growth factor 2 (IGF-2) is a protein growth hormones which share three structural similarity to insulin. The MeSH definition reads: "A well characterized neutral peptide believed to be secreted by the liver and circulate in the blood has regulatory and insulin-like growth factor mitogenic growth has an important, but not absolute, dependency, somatotropin (growth hormone, GH). Believed to be an important factor for growth of the fetus in contrast to the factor insulin-like growth factor-1, which is an important growth factor in adults. "In humans, the IGF-2 gene is located on chromosome 11p15.5, a region that contains a number of imprinted genes. The main role of the IGF-2 promoter is as a growth hormone during pregnancy. In the process of folliculogenesis, IGF-2 is created by thecal cells to act on the autocrine fashion thecal cells, and cells in a paracrine manner ovarian granulosa IGF-2 promotes proliferation of granulosa cells during the follicular phase the menstrual cycle, acting alongside follicle-stimulating hormone (FSH) to. After ovulation has already occurred, IGF-2 promotes the secretion progesterone during the luteal phase of the menstrual cycle, together with the luteinising hormone (LH). Thus, IGF-2 acts as a co-hormone, together with FSH and LH. A study in Monte Sinai School of Medicine found that IGF-2 may be connected to memory and playback.
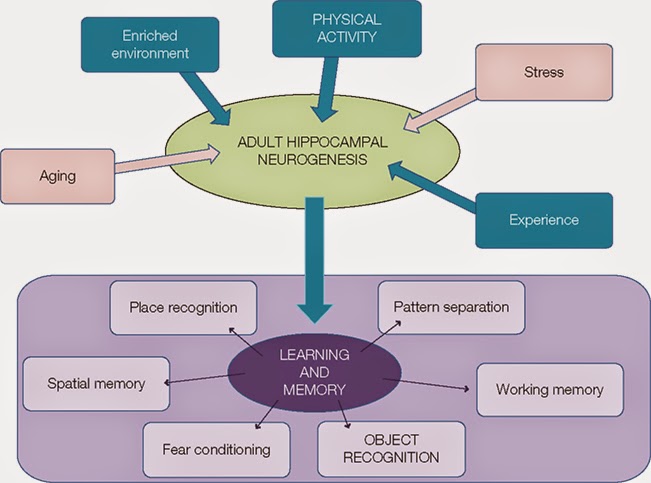
A study of European Neuroscience Institute, Goettingen (Germany) discovered that induced by fear extinction IGF-2/IGFBP-7 signaling promotes survival of 17-19 days old hippocampal neurons of newborns. This suggests that therapeutic strategies that enhance IGF-2 signaling and adult neurogenesis may be suitable for the treatment of diseases associated with excessive fear memory, such as PTSD (What is Posttraumatic Stress Disorder (PTSD)). When in danger, it's natural to feel afraid. This fear triggers many split-second changes in the body to prepare to defend against the danger or to avoid it. This response of "fight or flight" is a healthy reaction meant to protect a person from harm. But the disorder post-traumatic stress disorder (PTSD), this reaction is changed or damaged. People who have PTSD may feel stressed or frightened even when they are no longer in danger. The summary indicates that the impairment of IGF-2, during intrauterine growth, IGF-1 in the postnatal phase and GHD, entails a large impairment in several areas of metabolism, not only with growth deficiency at all stages but also compromises the central nervous system, maturation of the infant stage, including juvenile adulthood, and cognitive level. Moreover, the gold standard in development represents an excellent quality of life.
Dr. João Santos Caio Jr.
Endocrinologia – Neuroendocrinologista
CRM 20611
Dra. Henriqueta V. Caio
Endocrinologista – Medicina Interna
CRM 28930
Como saber mais:
1. É importante assinalar que podem existir fatores genéticos importantes e perceber que criança e infantil já apresentam alteração de lípides de forma precoce...
http://hormoniocrescimentoadultos.blogspot.com
2. Além do fator genético mesmo crianças com alimentação inadequada podem apresentar índices significativos de distúrbios lipídicos, o que antecipa eventuais comprometimentos vasculares principalmente cardíacos...
http://longevidadefutura.blogspot.com
3. Estudos tem comprovado que o GH também influencia positivamente e favoravelmente através do tratamento com GH rDNA tanto em crianças como em adultos...
http://imcobesidade.blogspot.com
AUTORIZADO O USO DOS DIREITOS AUTORAIS COM CITAÇÃO
DOS AUTORES PROSPECTIVOS ET REFERÊNCIA BIBLIOGRÁFICA.
Referências Bibliográficas:
Caio Jr, João Santos, Dr.; Endocrinologista, Neuroendocrinologista, Caio,H. V., Dra. Endocrinologista, Medicina Interna – Van Der Häägen Brazil, São Paulo, Brasil; Lacy KA, Parkin JM. A criança curto normal: estudo da comunidade de crianças em Newcastle-upon-Tyne. Arch Dis Child 1974 ; 49 : 417 -24; Greulich WW, Pyle SI. Atlas radiográficos de desenvolvimento do esqueleto da mão e do punho. 2a ed. Stanford, CA: Stanford University Press, 1959; Roche AF, Chumlea WC, Thissen D. Avaliação da maturidade esquelética da mão e punho: método Fels. Springfield, IL: Charles C Thomas, 1988; Tanner JM, Whitehouse RH, Cameron N, Marshall WA, Healy MJR, Goldstein H. Avaliação da maturidade esquelética e previsão de altura adulta. 2a ed.New York: Academic Press, 1983; Epstein LH, Asa RR, Valaski A. Infância obesidade. Pediatr Clin North Am1985 ; 32 : 363 -79; Forbes GB. Influência da nutrição. In: Forbes GB, ed. Composição do corpo humano: o crescimento, envelhecimento, nutrição e actividade. New York: Springer-Verlag, 1987: 209-47; Lifshitz F. Endocrinologia Pediátrica: um guia clínico. Nova Iorque: Marcel Dekker, Inc, 1996; Malina RM. A atividade física ea formação: efeitos sobre a estatura eo surto de crescimento adolescente. Med Sci Sports Exerc 1994 ; 26 : 759 -66; Malina RM. O crescimento físico e maturação biológica de jovens atletas.Exerc Esporte Sci Rev 1994 ; 22 : 389 -433; Theintz GE, Howald H, U Weiss, Sizonenko PC. A evidência para uma redução do potencial de crescimento em ginastas adolescentes. J Pediatr1993 ; 122 : 306 -13; Theintz GE. Endocrine adaptação ao treinamento físico intensivo durante o crescimento. Clin Endocrinol 1994 ; 41 : 267 -72; Constantini NW, Warren MP. Menstrual disfunção em nadadores; uma entidade distinta. J Clin Endocrinol Metab 1995 ; 80 : 2740 -4; Lindholm C, Hagenfeldt K, Ringertz BM. O desenvolvimento puberal em ginastas juvenis de elite.: Efeitos do treinamento físico Acta Obstet Gynecol Scand 1994 : 73 : 269 -73.Bernadot D, Czerwinski C. composição e crescimento do corpo seleccionados medidas de ginastas de elite júnior. J Am Diet Assoc 1991 ; 91: 29 -33.